
 *Essential notice: medRxiv publishes preliminary scientific reports that will not be peer-reviewed and, subsequently, mustn’t be considered conclusive, guide clinical practice/health-related behavior, or treated as established information.
*Essential notice: medRxiv publishes preliminary scientific reports that will not be peer-reviewed and, subsequently, mustn’t be considered conclusive, guide clinical practice/health-related behavior, or treated as established information.
In a recent study posted to the medRxiv* preprint server, researchers in Australia report the sturdiness and dynamics of recalled severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) spike (S) protein-targeted antibody-mediated immunity not less than eight months after breakthrough infection (BTI) with SARS-CoV-2 Omicron BA.1 and BA.2 subvariants.
Study: Durable reprogramming of neutralising antibody responses following breakthrough Omicron infection. Image Credit: Nemes Laszlo / Shutterstock.com
Background
The continual emergence of highly transmissible and immune-evasive Omicron subvariants, coupled with the waning of coronavirus disease 2019 (COVID-19) vaccine-elicited immunity, has increased BTI frequency amongst COVID-19 vaccinees. Previous studies on memory B lymphocyte- and antibody-mediated responses post-SARS-CoV-2 Delta or BA.1 BTIs have shown rapid anti-S humoral response recall, S-targeted memory B lymphocyte reactivation, and antibody-secreting cell differentiation.
Moreover, Omicron BTIs amongst fully vaccinated individuals enhance neutralization breadth, possibly attributable to novel antibodies targeting Omicron S epitopes or selective cross-protective memory B lymphocyte re-expansion during vaccination.
Evaluating the influence of BTIs with novel Omicron subvariants on the breadth and sturdiness of humoral and memory B lymphocyte-mediated immunity could inform optimized vaccine development for max protection from emerging SARS-CoV-2 infections.
In regards to the study
In the current study, researchers evaluate the initial recalled immune response kinetics after BA.1 or BA.2 BTIs and profiled alterations in SARS-CoV-2 neutralization post-recovery.
Twenty-six COVID-19 vaccinees, consisting of three fully vaccinated and 21 booster-vaccinated individuals and two individuals with prior SARS-CoV-2 ancestral strain infections who were subsequently vaccinated, were enrolled following Omicron BTIs occurring after a median of 95 days of receiving probably the most recent vaccination.
Among the many study participants, 19 of 21 individuals had no history of SARS-CoV-2 infection and were vaccinated with S protein-encoding COVID-19 vaccines resembling ChAdOx1 nCoV-19, BNT162b2, NVX-CoV2373, and messenger RNA (mRNA)-1273.
BA.1 infections were confirmed by whole genome sequencing (WGS). As well as, the nasal cavity and blood of the participants were sampled for not less than 247 follow-up days.
SARS-CoV-2 ribonucleic acid (RNA) levels were determined using a quantitative polymerase chain response (qPCR) assay for the SARS-CoV-2 nucleocapsid (N) gene. Anti-Omicron neutralization was modeled to estimate the sturdiness of immune protection against symptomatic reinfections with equivalently or more immune-evasive SARS-CoV-2 variants of concern (VOCs) amongst individuals with hybrid immunity.
Linear mixed effects modeling was performed to estimate the typical decay rate. BTIs were diagnosed using rapid antigen tests and PCR, whereas anti-N titers were determined using enzyme-linked immunosorbent assays (ELISA).
The ancestral SARS-CoV-2 strain was cultured on Vero cells, whereas BA.1, BA.2, and BA.4 subvariants were grown on Calu3 cells. SARS-CoV-2 infectivity was assessed using HAT-24 cells expressing human angiotensin-converting enzyme 2 (ACE-2) and transmembrane serine protease 2 (TMPRSS2).
Percent viability and neutralization were determined based on the relative fluorescent units (RFU) values, and the mean ID50 values and IC50 values were determined. Flow cytometry was performed to detect SARS-CoV-2 S-targeted B lymphocytes, with modeled antibody recall and decay kinetics. Vaccine efficacy against different VOCs following BTI was estimated.
Results
All study participants developed symptomatic but mild BA.1 or BA.2 BTIs. These infections robustly enhanced their neutralization breadth against the causative VOCs, thereby expanding neutralization breadth against the more immune-evasive BA.4.
Cross-reactive memory B lymphocytes against the ancestral and Omicron S proteins were mainly expanded by SARS-CoV-2 infection, with limitedly recruited Omicron-targeted B lymphocytes or anti-SARS-CoV-2 antibodies de novo.
Modeling estimates indicated that immune protection against symptomatic reinfections with closely related VOCs would have considerable durability but could be undermined by novel and increasingly immune-evasive VOCs. Follow-up analyses indicated durable anti-Omicron neutralizing responses.
BA.1 and BA.2 BTIs showed comparable SARS-CoV-2 kinetics, with most infected individuals exhibiting peak viral loads at enrollment and up to 3 days following the onset of symptoms. SARS-CoV-2 replicated robustly during Omicron BTIs, despite previous vaccinations.
Serological anti-N immunoglobulin G (IgG) titers were negligible on the initial time points; nonetheless, the titers consistently expanded from one week after symptom onset of BA.1 and BA.2 BTIs. Immune protection was estimated to be over 70% and last for 705 days and 1,607 days after BA.1 and BA.2 BTIs, respectively.
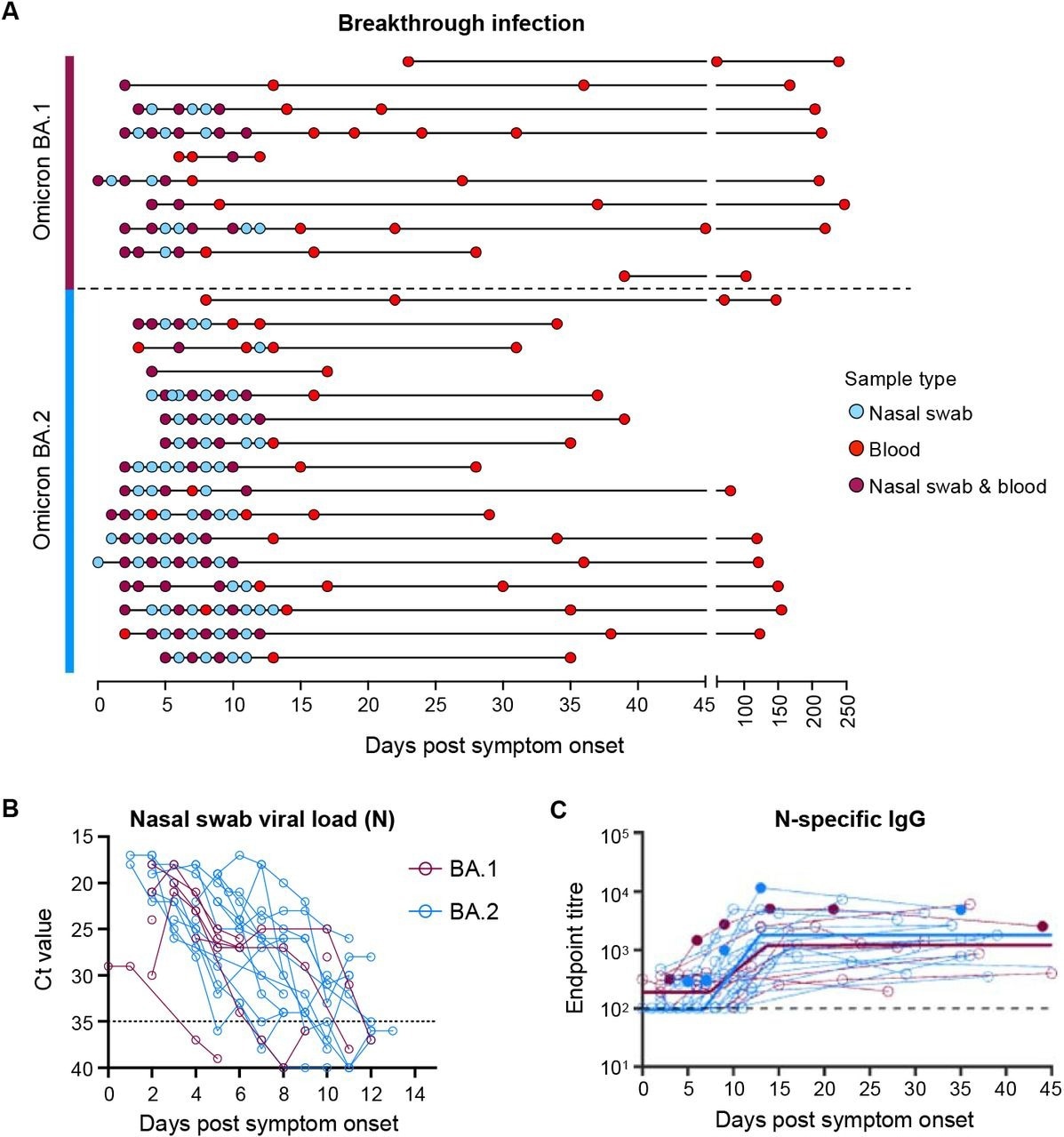
Viral load kinetics and seroconversion to N following Omicron BA.1 and BA.2 breakthrough infection. (A) Schematic of longitudinal sample collection following breakthrough infection of vaccinated individuals with Omicron BA.1 (n=10) or BA.2 (n=16). Each line represents a single subject, and every point represents a sample collection (blue, nasal swab; red, blood; purple, each nasal swab and blood). (B) Kinetics of SARS-CoV-2 viral load in nasal swabs measured by qPCR of the nucleocapsid (N) gene. (C) Kinetics of plasma IgG titers against SARS-CoV-2 nucleocapsid (N) following breakthrough infection with BA.1 (red) or BA.2 (blue). Subjects with previous SARS-CoV-2 infection are depicted in closed circles. The thick lines represent the mean estimate from the piecewise linear regression model using the estimated parameters.
Even during maximal SARS-CoV-2 neutralization, about one month following symptom onset, recent VOCs with three- and 10-fold lower neutralization could lower the efficacy of immune protection from 90.0% to 74.0% and 47.0%, respectively. Amongst individuals with hybrid immunity from BA.1 and BA.2 BTIs, protective efficacy would cut back from 95.0% to 86.0% and 63.0%, respectively.
Recovery from Omicron BTIs conferred markedly durable immune protection from antigenically similar strains; nonetheless, the protection might be subverted rapidly by the emergence of more immune-evasive VOCs.
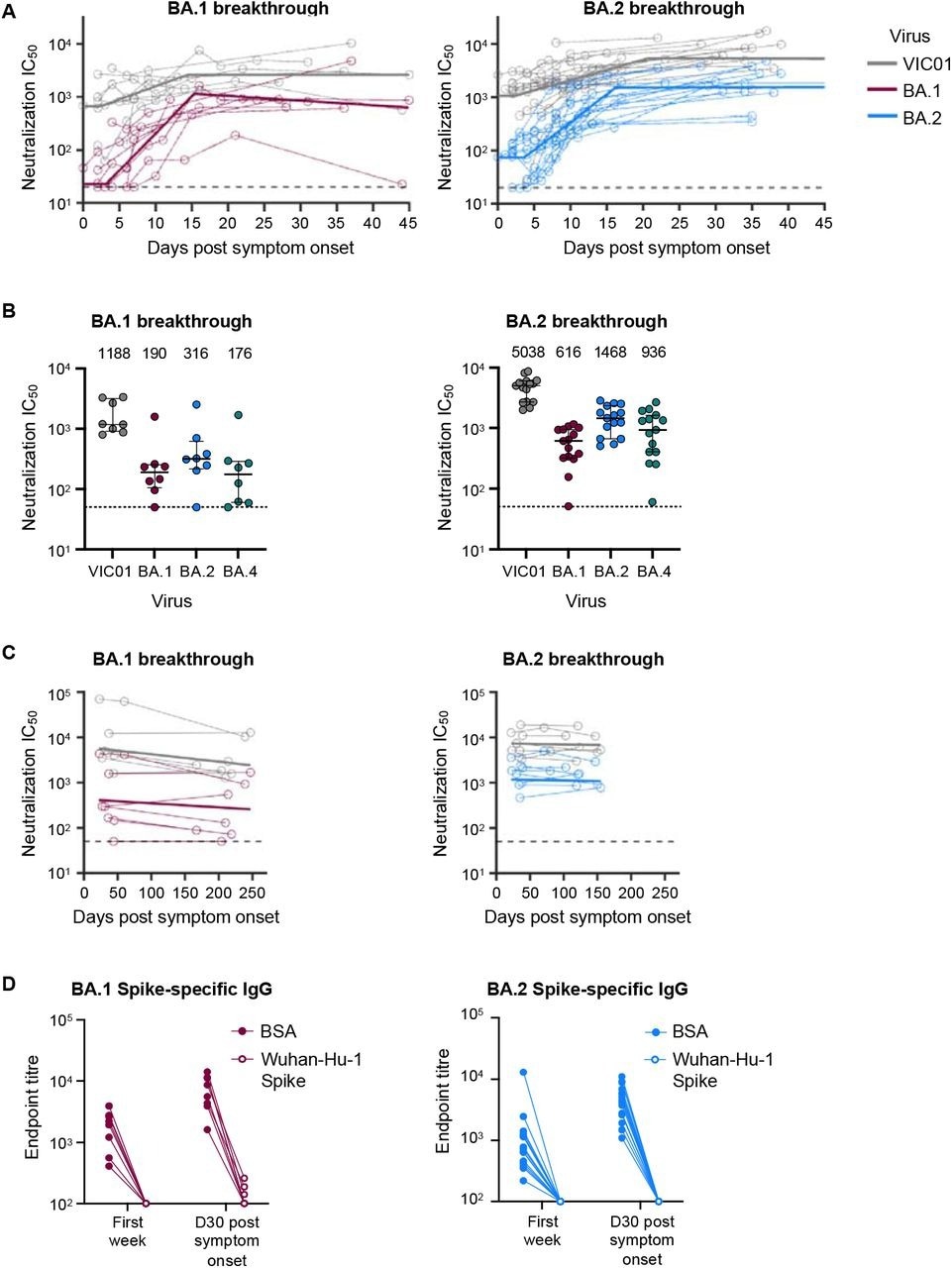
Omicron BA.1 and BA.2 breakthrough infection rapidly recalls neutralising antibodies which are broad and sturdy. (A) Kinetics of plasma neutralization activity following breakthrough infection against ancestral VIC01 or matched infecting Omicron BA.1 and BA.2 strains. Thick lines represent the mean estimate from the piecewise linear regression model using the estimated parameters. Plasma neutralization activity was measured using a live virus neutralization assay against SARS-CoV-2 clinical isolates in HEK293T cells transduced with ACE2 and TMPRSS2. (B) Neutralization mediated by BA.1 and BA.2 breakthrough plasma against ancestral VIC01, Omicron BA.1, BA.2, and BA.4 strains at a median of 34 days post-symptom onset. Data are presented as median ± IQR. (C) Longitudinal decay kinetics of plasma neutralization activity following breakthrough infection against ancestral VIC01 or matched infecting Omicron BA.1 or BA.2 strains as much as 4-7 months post-symptom onset. The very best-fit decay slopes (thick lines) are depicted. (D) IgG antibody endpoint titers against BA.1 spike for BA.1 breakthrough subjects (red) and against BA.2 spike for BA.2 breakthrough subjects (blue) following pre-incubation with BSA control (closed circles) or ancestral Wuhan-hu-1 spike (open circles).
The team estimated that 70% protective efficacy for the SARS-CoV-2 homologous strain might be maintained for nearly 4.5 and 7 years for BA.1 and BA.2 BTIs, respectively. Likewise, durable immune protection for the SARS-CoV-2 ancestral strain was estimated to persist for over 8.5 years and 10 years for BA.1 and BA.2 BTIs, respectively.
Conclusions
Omicron BTIs were found to induce durable neutralizing immune responses by recalling cross-reactive and vaccine-induced memory B lymphocytes.
*Essential notice: medRxiv publishes preliminary scientific reports that will not be peer-reviewed and, subsequently, mustn’t be considered conclusive, guide clinical practice/health-related behavior, or treated as established information.